What is the carpal tunnel?
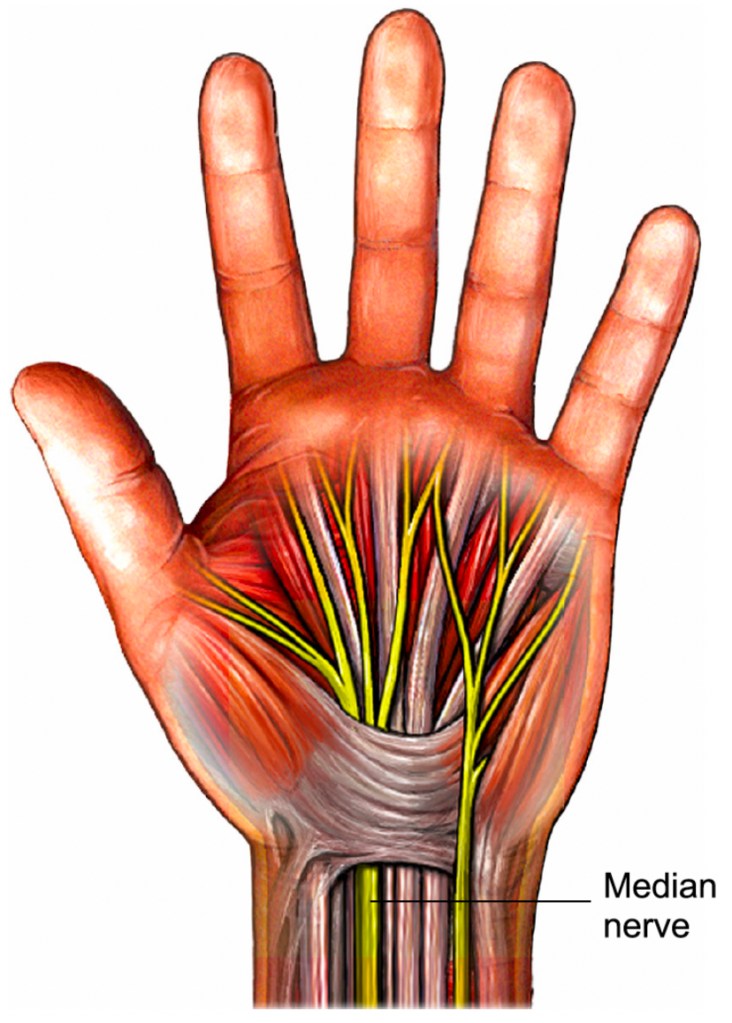
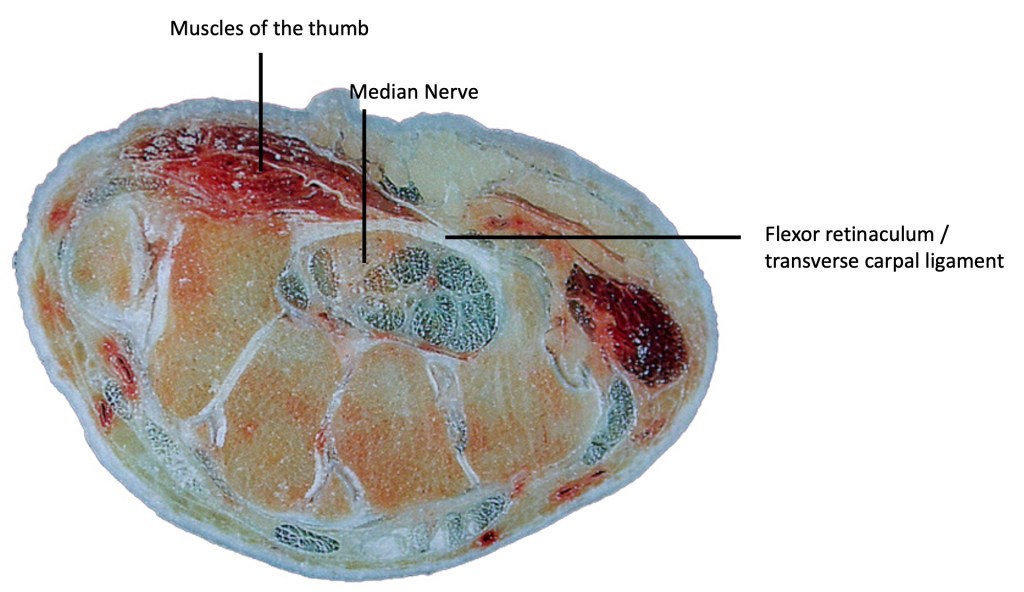
The carpal tunnel is a canal formed between the small bones of the wrist called carpal bones and a ligament that lies across the front of the wrist. The ligament is known as the flexor retinaculum or the transverse carpal ligament. A large nerve (the median nerve) and the tendons that bend the fingers and thumb pass through this tunnel. The nerve supplies sensation to the fingers, and some of the hand muscles (diagram below).
What is carpal tunnel syndrome?
Carpal tunnel syndrome (CTS) is a condition where the large nerve (the median nerve) is compressed as it passes through the tunnel at the wrist. CTS may be associated with swelling in the tunnel which may be caused by inflammation of the tendons, a broken wrist bone (fracture), wrist arthritis and other less common conditions. In most cases, however, the cause is unknown.
CTS commonly affects women aged in their 40’s and 50’s but can occur at any age in either sex. CTS can occur during pregnancy and with conditions such as diabetes, thyroid problems, rheumatoid arthritis and other less common conditions. Most patients have none of these, and this is known as idiopathic carpal tunnel syndrome.
What are the symptoms?
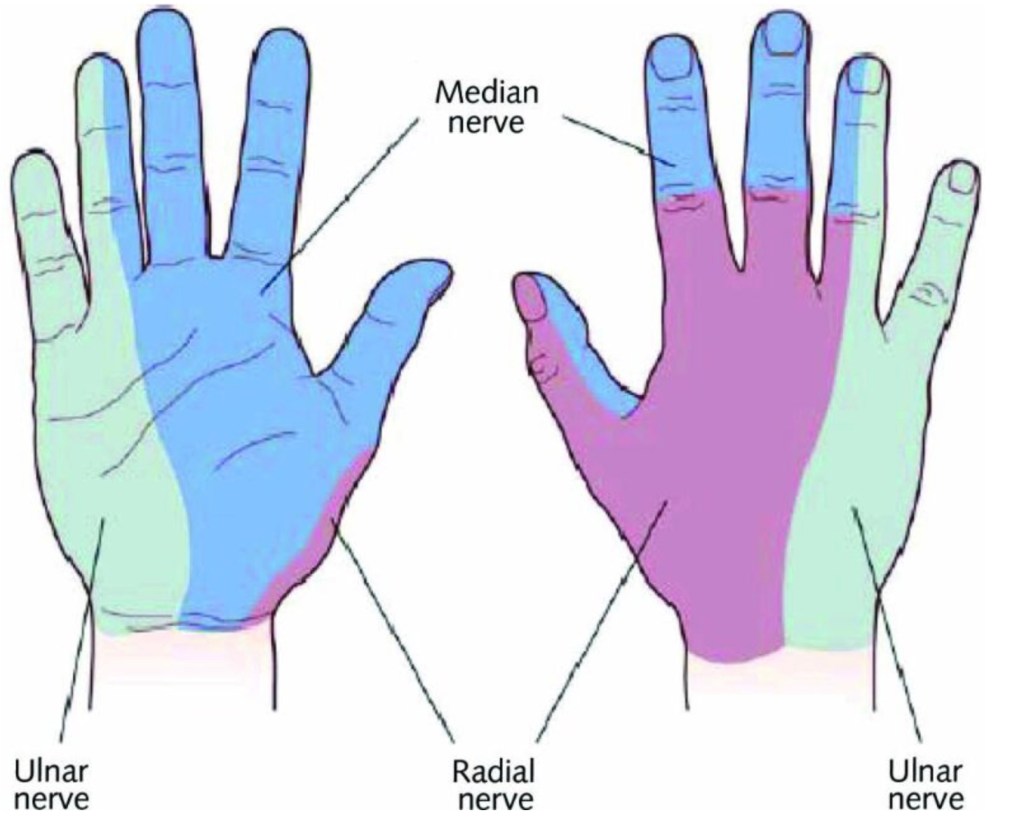
The main symptom is altered feeling in the hand, affecting the thumb, index, middle and ring fingers. It is unusual for the little finger to be involved. Many people describe the altered feeling as tingling. Tingling is often worse at night or first thing in the morning. It may be provoked by activities that involve gripping an object, for example a mobile phone. People may notice tingling now and again and then sensation will return to normal. As time goes on the altered feeling may become continuous, with numbness in the fingers and thumb. There may be weakness and wasting of the muscles at the base of the thumb. Patients often describe a feeling of clumsiness and drop objects easily. Patients can also have pain in the wrist and forearm.
How is it diagnosed?
In many cases the diagnosis can usually be made based on patient symptoms and examination. There are 2 tests used by surgeons to help make the diagnosis: Phalen’s test is a simple manoeuvre where the wrist is allowed to flop down with gravity when the elbow in on a table. This manoeuvre increases the pressure within the carpal tunnel, and in patients with carpal tunnel syndrome this will give rise to tingling in the area supplied by the median nerve. Some surgeons may add some compression over the wrist whilst bending the wrist down.

Tinel’s sign involves lightly tapping over the nerve to detect an area of irritation. This will produce a tingling sensation in the hand if the test is positive.
A test to measure nerve impulses (nerve conduction study) will usually confirm the diagnosis, and give an idea as to how severe the problem is. This study involves a doctor or specialist technician placing some sticky pads on the arm and measuring the speed taken for signals to be transmitted down the nerve. It can feel uncomfortable but is not usually painful.
What is the natural history
In many patients, symptoms from carpal tunnel syndrome can come and go for some time before either settling down or becoming a problem. If there is an underlying cause such as diabetes or thyroid disease, pregnancy, or even menopause in women, then treating this condition may help resolve symptoms. CTS due to pregnancy often will get better after the baby is born.
If there has been a trigger such as a work related or sporting activity then making changes to these activities can help settle symptoms. If the condition continues to worsen, there is a risk of losing function in the hand, with the median nerve not working. This gives a permanent numbness in the hand, and weakness of thumb movement. People worry about deterioration of function, but it usually goes hand in hand with symptoms, so that there is usually plenty warning of deterioration in the function of the median nerve.
What is the treatment
1) Splinting – A wrist splint with the wrist in a straight position is usually the first step in treatment. The splint should be worn for 2-3 months, usually at night. Activities which provoke the symptoms should be avoided if possible. Buy a wrist splint here.
2) Steroid Injection – A steroid injection into the carpal tunnel may be useful in selected patients. Steroid is thought to work by reducing any inflammation within the carpal tunnel, but is also known to breakdown fat and connective tissue, leaving more space within the tunnel. Steroid injection can be recommended if nerve studies show that the condition is very mild, or if there are reasons why surgery to the hand would cause problems at work or for other reasons. Steroid injections can be used to support a diagnosis of CTS if there is any doubt in diagnosis. Having a steroid injection
3) Surgery – Surgery remains the most effective, proven long-term solution to Carpal Tunnel Syndrome. The operation involves cutting the ligament over the front of the wrist to ease the pressure on the nerve. The surgery is routinely done under local anaesthesia.
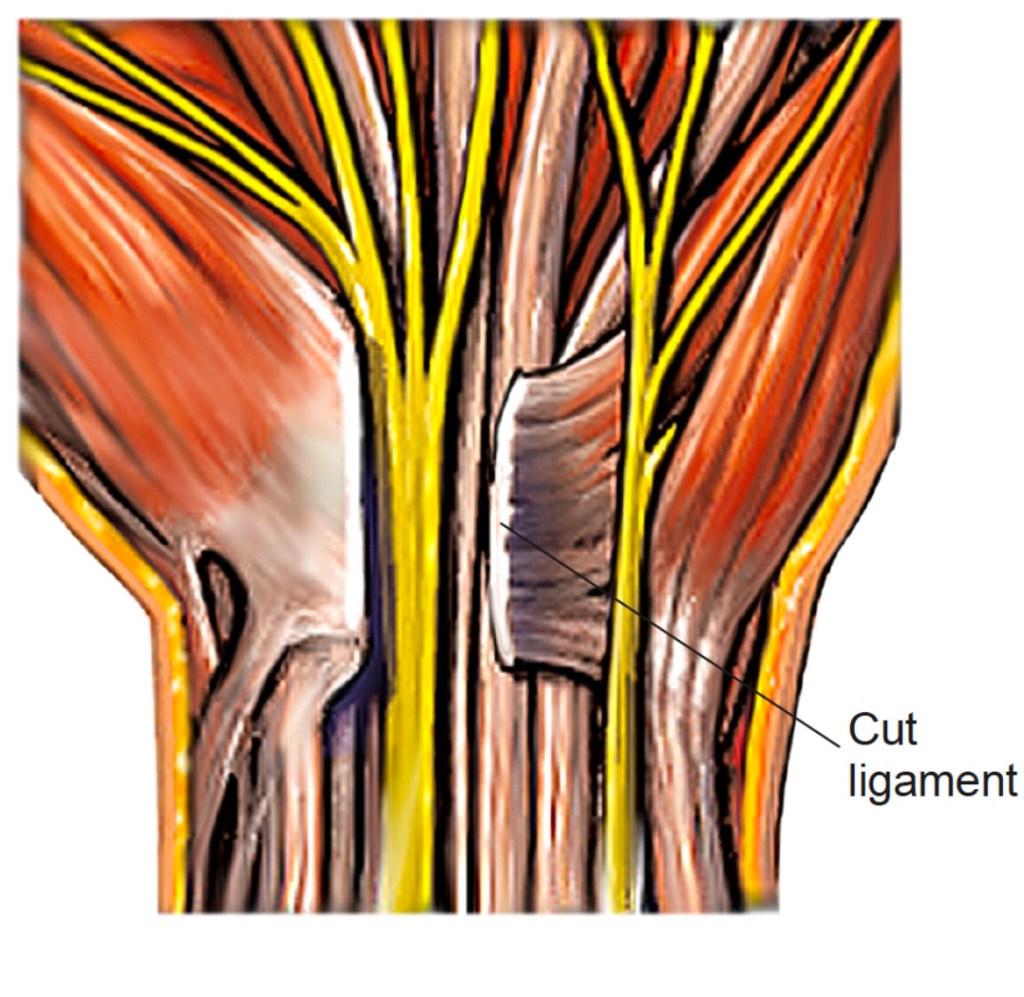
This usually cures the problem. Night pain and tingling usually disappear within a few days. In severe cases, constant numbness and muscle weakness may be slow to get better or may not be much better than before surgery. Occasionally pain can be felt over the inside of the wrist. It generally takes about three months to get back full strength and a comfortable scar. The hand can be used for light activities from the day of surgery.
Although surgery is a relatively safe option with excellent 1 year outcomes, there is a price to pay. Since the surgeon divides the ligament at the front of the wrist (flexor retinaculum / transverse carpal ligament), the normal function of this ligament is lost. There are 3 consequences of losing the ligament:
- The wrist joint loses one of its stabilising ligaments. This can result in a feeling of instability when using the hand for anything heavy, or a dull ache across the base of the hand when pushing up from a chair or bath. In patients with pre-existing arthritis of the wrist, arthritic symptoms can be exacerbated by loss of the ligament. These symptoms improve with time and are generally not an issue at the one year follow up.
- The flexor tendons (tendons responsible for grip) lose one of the ‘pulleys’ used to increase their efficiency. Loss of the ligament usually results in loss of grip strength, although this recovers over the course of around 1 year, and is usually normal in the long term.
- The small muscles of the hand that work the thumb and little finger normally pull from the ligament. When the ligament is divided, these muscles immediately pull on something unstable, making pinch grip difficult for the first few weeks. Again, this tends to improve with time and returns to normal within a year.
Overall, the results of open carpal tunnel decompression are excellent with around 96% of patients reporting good outcomes at 1 year. There are risks involved with all surgery, however, and you can read more about these risks here

© Lothian Virtual Hand Clinic 2023
