What is the volar plate?
The small joints of the hand are designed to flex or bend to form a fist. For this reason, the tissue over the back of the joint is very flexible and loose to allow full flexion, whereas the tissues at the side of the joint and on the palm side have to provide the joint with the stability it needs for normal hand function.
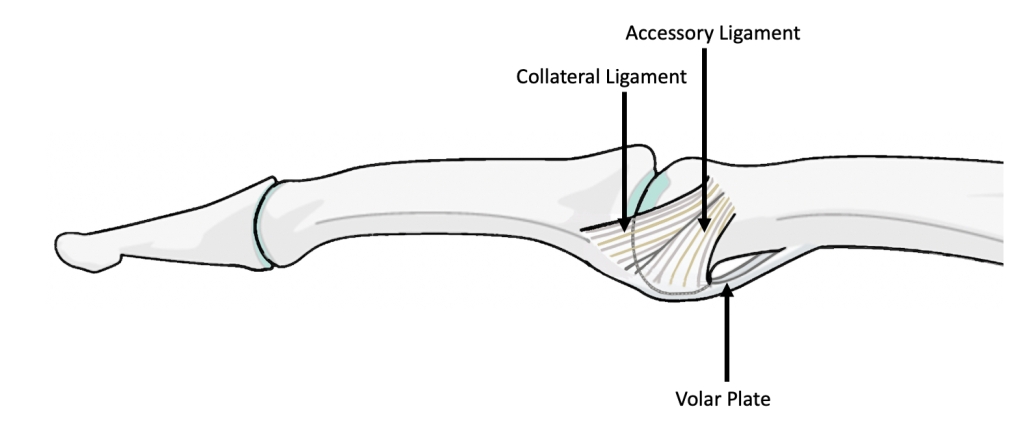
Each joint is restrained by a thick ligament on either side of the joint (collateral ligaments), and a structure called the volar plate, which sits at the front of the joint and prevents hyper-extension of the finger. The volar plate is made of a tough fibrocartilage and is a few mm thick. It has a built in mechanism to allow the joint to fully flex, but tightens up when the joint is straightened, and becomes fairly rigid with full extension of the joint.
How is the volar plate injured?
The volar plate and collateral ligaments are injured when a force is applied to the finger that bends it backwards (hyper-extension) or to the side. A good example is when a goal-keeper puts his hand out to save a ball, and the force of the ball hyper-extends the finger, tearing the volar plate and injuring the ligaments. The injury is common in baskeball players and goalies, but also commonly occurs from a fall onto the outstretched hand, where the finger takes the brunt of the force.
What types of injury can occur?
Volar plate injuries can impact on the overall stability of the knuckle joint. It is impossible to get this injury without disrupting the joint, and depending on the force applied, this can be minor, or can be enough to dislocate the joint. The injuries can be divided into 2 types:
STABLE – Most volar plate injuries are stable, meaning that the structures within the joint maintain their normal relationship with each other and do not appear deformed (although they may appear swollen). The bone contours and pull of the tendons keep the joint in place, and it is quite safe to mobilise the finger without fear of damage to the joint. If there is an associated fracture or break in the bone where the volar plate is attached, it is small and does not impact on joint stability.

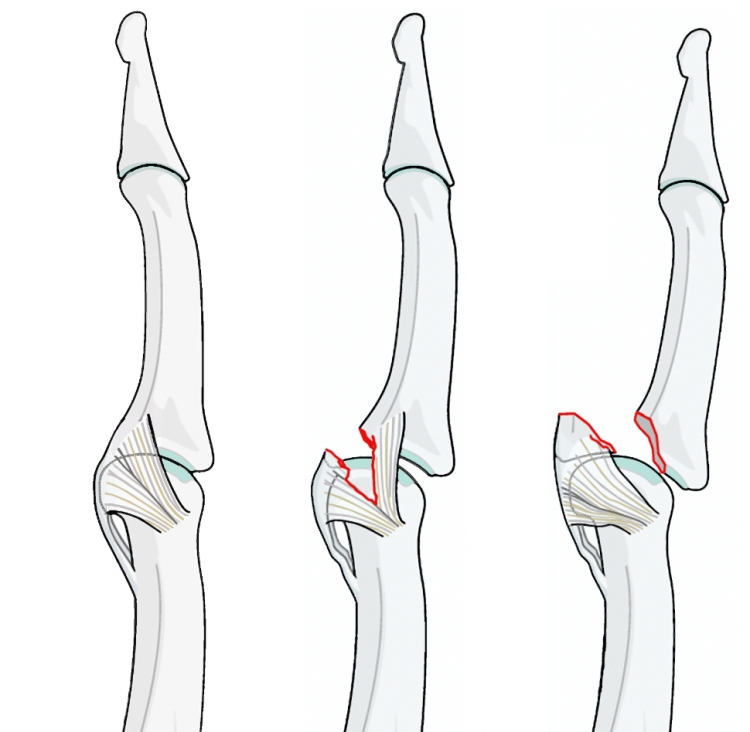
UNSTABLE – In an unstable injury, there is a risk of dislocation or subluxation of the joint (partial dislocation). There is often a fracture or break of the bone where the volar plate is attached which involves over 1/3rd of the joint surface. The joint can also be unstable if the collateral ligaments have stripped off the bone.
What are the symptoms and signs of a volar plate injury?
When the volar plate tears off the bone, there is bleeding around the joint, and the joint becomes very swollen. Because of the increased pressure from the bleeding, it is also very painful and usually will not move much without pain.
What is the treatment?
STABLE INJURIES – The vast majority of volar plate injuries are stable, and can be safely moved. The finger may be strapped to the finger next door for the first week or two to provide it with a splint, but this is not necessary for treatment. Finger flexion (or bend) usually starts to return within a week or two, but can take a few months to return to normal. Finger extension (straightening) is often slow to return fully, and has to be worked at by forcibly straightening the finger over the first month or two. The joint is usually very swollen for many weeks, and it is usually around 8-12 months before the normal skin creases reappear on the back of the joint.
UNSTABLE INJURIES – Unstable injuries can be difficult to treat. Usually, surgery is recommended to make the joint stable, and then the joint can be treated in the same way as a stable injury. Surgery may involve simply putting a metal pin into the back of the finger to prevent dislocation. Depending of the degree of injury, open surgery to assess the joint to repair the torn structures may be needed.
What is the outcome?
When the soft tissues around the joint heal, it is with scar tissue rather than the type of tissue that has been injured, and scar tissue is far more bulky than normal tissue. Scar tissue contracts down with time, so that all scars end up looking and feeling much smaller than the initial scar. The same is true in the finger, and although the swelling will slowly go down, the finger almost never gets back to the same size it was before the injury. The vast majority of patients get back full function in the finger, with a slight bend to finger that was not present before the injury.
Stiffness – Sometimes the finger becomes stiff following this injury, despite best efforts to mobilise the joint. This can be treated with physiotherapy, but occasionally the stiffness may be permanent.
Residual pain – This is common up until around a year following the injury, but people rarely complain of long term pain in the finger.
Arthritis – A small proportion of people with a volar plate injury develop arthritis in the joint.
What exercises should be done?
Simple bending and straightening exercises are usually enough here. These should be done regularly – every 15 mins or so, with 10 repetitions each time.
Proximal Phalangeal Joint fracture (PIPJ): However, complex fractures often require open surgery to reduce and hold the fracture, opening the joint to repair the torn structures. Sometimes small amount for bone graft need to be taken from the distal radius, via a separate incision on the back of the wrist. These complex fractures with injury to the small PIP joints in the finger, often require surgery to re-align the joint. a common problem following surgery is the risk of stiffness. Thus significant commitment by the patients to do their hand therapy exercises regularly and enthusiastically after the surgery is essential to give the best possible movement.
Hemi-hamate arthroplasty: is a reconstruction option for severe fractures to the volar part of the middle phalanx at the PIPJ. If your injury is significant, this and other reconstructive surgical options will be discussed by your surgeon.

© Lothian Virtual Hand Clinic 2023
